Dental Implants Systems**************UPDATE 2013**********
We are now using Co-Axis and Max implants from Southern Implants. These are angulated and large diameter implants that can eliminate the need for bone grafting or vastly reduce the amount of bone grafting needed for most implant patients. This reduces post operative discomfort, expense, and number of surgeries needed. Thank to these innovations unique to southern implants and make a remarkable difference to enhance treatment experience and outcomes and lower costs. Check out this Video http://vimeo.com/23853066
*********************************
Are there different implants used?
Just like with any technology dental implants come in various brands. There are about 70 different brands available worldwide with over 2000 different implant systems. Most implants are made from commercially pure titanium or titanium alloy and have various geometry, surface treatments and ways to connect teeth the the implant.
Is any one system better than another? While in general all implant systems will integrate to the bone, the accuracy that they are manufactured with, the engineering tolerances and the surface treatment and cleanliness are important factors in long term success. The way the teeth are connected to the implant and the strength of the connection, availability of components in the future, the strength to prevent flowering of the metal during insertion of the implant or abutment and the soft tissue response to the collar are also important factors.
What implant system are used in Dublin Specialist Dentistry?
Mr Rogers and Dr. Fitzgerald have extensive experience with many implant systems including Branemark System, Nobel Biocare, Ankylos, Biomet 3i, Straumann and Southern Implants. These are all large manufacturers having been in business for 20 or more years. These systems have all proven on average 95% success rates in the dental literature. The components are easily available and will continue to be in the future. Also a number of components are interchangeable between these systems.
In Dublin Specialist Dentistry we favour Southern Implants. This implant system has evolved since 1987 (this first commercially available implant came on the market in 1981) and avoids the flowering issues, fixture mount fractures and restorative issues found with other systems. They are made from strengthened commercially pure titanium and the engineering tolerances are superior to many of the other big brands (1). The surface is a sandblasted moderately rough surface. This implant system is used worldwide by many of the teaching institutions in the US and has literature of great enough longevity and quality to be included in the 2005 Cochrane review (11) on implant success rates. This review stated that there are over 70 Dental Implant Manufacturers in existence. Only 4 of these Manufacturers have the necessary High Level data to prove efficacy of use over a 5 year period. These are Southern Implants, Nobelbiocare, Straumann and Astra.
One nice feature of the Southern Implant system is that the connection is available in external, and 2 internal configurations. Also there are angled implants and very wide implants for sites with minimal bone.
Our success rate, in our clinic for our patients with this implant system is over 98% in our 2011 clinical audit.
UPDATE : Southern Implants has launched the Co-Axis and Max dental implants. These design modifications allow implants to be placed for more people, at a lower cost with less bone grafting and in shorter time frames. More info here
Should I be concerned about the implant system used?
Yes this is a medical implant that will be inserted into your body. Implants must have good long term research, clean well prepared and well researched surfaces, reliable well researched connections and restorative versatility in the future. It is your surgeons & prosthodontists job to select and use a quality system in your mouth. We have such faith in the systems that we use, that any failed implants will be replaced free of charge. We have placed Southern Implants in our own family's mouths. The factors which define success are much more reliant on the treatment planning and skill of the surgeon and prosthodontist. We have read the scientific literature not just company marketing or non peer reviewed internet abstracts.
Will Components be available for my implants in the future?
The connection system we favour is the tri-nex internal connection from Southern Implants. We also use external hex implant for certain cases and this connection has been available for 40 years. We see implants placed in other clinics for which we cannot get components or that components have to be shipped in at great expense. This will never be the case for the implants we place.
Are implant surfaces important?
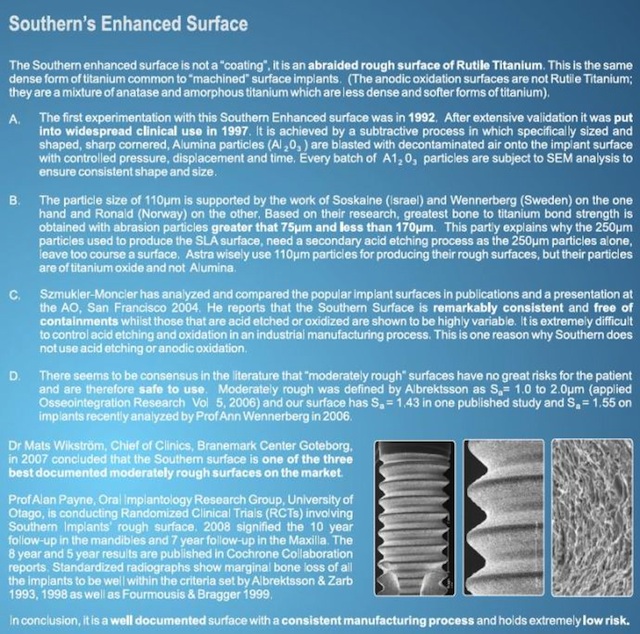
Yes, there are better results with moderately rough implant surfaces as compared to the 1980 smooth surface implants. There are new bioactive surfaces and surface treatments. However at Dublin Specialist Dentistry we are not happy to use technology with only short term data on our patients and we stick to the moderately rough subtractive surface with proven excellent success rates. The details of the surface we use is outlined below. Southern Implants provide over 12 years of data on their current surface, this is more than any other manufacturer for their current surface.
.
.
 .
I want "X" Brand of implant will you place this for me?
No we do not offer different standards of care for different patients. All our patients receive what we feel is the best care. We would not use an implant that was in any way inferior to another, we do not offer a "budget implant". When we place an implant we are just as concerned about the long term success of it as you are.
I have been told by another dentist that the implants they use are superior?
This simply is not correct. Having 20 years experience between them Dr. Fitzgerald and Mr. Rogers have seen implants which have failed, and implants that have been successful from nearly every common system. Any analysis of the 30 years of modern implant literature fails to show that any system is superior to another. It is also notable that some of the companies who claim to have superior implants have had to remove heavily marketed and under researched products from the market due to poor clinical performance. The success is much more dependent on who places and restores the implant than any factor associated with the implant itself. It is much more important to choose a clinician who has the training, knowledge of the literature and knowledge of the history of implants to know what is marketing spin and what really works. And who is cautious enough not to try unproven techniques or products on you.
Can I have cheaper mini dental implants?
We use mini implants only as temporary implants to support teeth during treatment, these are removed once the temporary is no longer needed. Mini implants have shown unacceptably high failure rates which are not suitable for our patients.
Literature
1. Dellow, A.G., Driessen, C.H., Nel, H.J.C. Scanning Electron Microscopy evaluation of the interfacial fit of interchanged components of four dental implant systems. Int J of Prosthodont 1997 10; 216-221. The introduction of the original Swedish implant system (Branemark) was followed by several alternative implant systems with implants and components that closely resembled the original design and treatment protocol. Some of these alternative systems may be interchangeable. Manufacturing variations can result in as much as 0.1 mm of space between the component parts. The implant/abutment interface fit was evaluated by scanning electron micrography for each of four implant systems, as well as interchanged components between the various systems. Results showed that certain implant system abutments are interchangeable and that the accuracy of fit meets with or exceeds the criteria set by the original Swedish system. 2. Tawse-Smith, A., Payne, A.G.T., Kumara, R., Thomson, W.M. One-stage operative procedure using two different implant systems: A prospective study on implant overdentures in the edentulous mandible. Clin Implant Dent Relat Res 2001; 3-4; 185-193. BACKGROUND: Evidence-based reports are needed to support the application of a one-stage surgical protocol for unsplinted implants supporting mandibular overdentures. PURPOSE: To examine the feasibility and success of using two different dental implant systems (originally designed for two-stage operative technique) using a one-stage operative procedure in patients being rehabilitated with implant supported mandibular overdentures. MATERIALS AND METHODS: The study sample involved 24 edentulous subjects (aged 55-80 yr) randomly allocated to two different implant systems, one with a machined titanium implant surface (Steri-Oss/Nobel Biocare, Goteborg, Sweden) and the other with a roughened titanium surface (Southern Implants, Ltd., Irene, South Africa). Two unsplinted implants to support implant overdentures were placed in the anterior mandible of all patients, using a standardized one-stage surgical and prosthodontic procedure. Primary stability and bicortical anchorage of the implants was mandatory before healing abutments were connected at the time of implant placement. Implant overdentures and their respective matrices were inserted following a standard 12-week healing period. Data relating to mobility tests, radiographs, and peri-implant parameters were documented at 12, 16, and 52 weeks after surgery. RESULTS: A success rate of 95.8% for the Steri-Oss and 100% for the Southern Implants was found, without any statistically significant differences in the marginal bone loss. Significant changes in Periotest values were observed for both types between 12 and 52 weeks (p < .001). Minor changes were observed in the peri-implant parameters evaluated. CONCLUSIONS: These preliminary findings show a successful application of this one-stage approach for unsplinted implants supporting mandibular overdentures with Steri-Oss and Southern Implant Systems. 3. Tawse-Smith, A., Payne, A.G.T., Kumara, R., Thomson, W.M. Early loading of unsplinted implants supporting mandibular overdentures using a one-stage operative procedure with two different implant systems: A 2-year report. Clin Implant Dent Relat Res 2002; 4: 33-42. This article is a 2 year follow-up on the above article. BACKGROUND: Step-wise reduction in loading protocols is necessary to evaluate early loading of implants with mandibular overdentures. PURPOSE: To compare the success rates of two different dental implant systems following conventional or early loading protocols in patients being rehabilitated with mandibular overdentures. RESULTS: There was no statistically significant difference in the success rates of the two systems in either control or test groups. At the 2-year evaluation, a success rate was found of 87.5% and 70.8% for the control and test Steri-Oss groups, respectively, and 83.3% and 100% for the control and test Southern Implants groups were observed. For the Steri-Oss groups, eight implants were lost at an early stage: seven in the test group and one in the control group. For the Southern Implants control and test groups, no failures were seen at any time interval. There were no significant differences in marginal bone loss, Periotest values, and peri-implant parameters between implant systems or between any of the control or test groups. CONCLUSIONS: Early loading, with step-wise reductions in loading protocols, of unsplinted machined Steri-Oss and roughened Southern Implants fixtures with mandibular overdentures is possible for up to 2 years. 4. Boyes-Varley, J.G., Lownie, J.F., Howes D.G., Blackbeard G.A. Surgical modifications to the Branemark Zygomaticus Protocol in the treatment of the severely resorbed maxilla: a clinical report. Int J Oral Maxillo Facial Implants 2003 PURPOSE: The Zygomaticus dental implant, designed by Nobel BioCare, was developed for the treatment of the severely resorbed maxilla. Branemark has reported an overall success rate of 97.6% with the placement of 183 implants over the last 12 years. The purpose of this article was to present a modification to the original Branemark surgical approach to achieve better access and optimal implant placement. MATERIALS AND METHODS: There are parameters within the patient’s resorbed skeletal frame that guide the surgical placement of the currently used implant however, there are shortcomings in the current surgical protocol. This report describes a simplified surgical approach in 45 patients (77 implants) using an implant with a modified head angulation of 55 degrees and a placement appliance to assist the surgeon in placing the implant as close to the crest of the edentulous ridge as possible. RESULTS: The placement appliance identifies accurately the anatomic constraints of the resorbed skeletal frame that limit implant placement. This, together with the modified surgical protocol, has resulted in improved access and in ideal positioning of the restorative head. DISCUSSION: The present technique allows restorative clinicians to achieve a more ideal restorative result in the posterior maxillary alveolus using the zygomatic implant, while reducing the buccal cantilever, improving tongue space, and access for maintenance. CONCLUSION: By placing the implant closer to the crest of the alveolar ridge using the placement appliance and an implant with a 55-degree head, the emergence of the restorative head and resultant buccal cantilever can be reduced by as much as 20%. 5. Nikellis, I., Levi, A., Nicolopoulos, C. Immediate loading of 190 endosseous dental implants: a prospective observational study of 40 patient treatments with up to 2-year data. Int J Oral Maxillofac Implants. 2004 Jan-Feb; 19(1):116-23. PURPOSE: The present study was undertaken to determine the feasibility of using primary stability as a predictor of implant success in patients whose implants were immediately loaded. MATERIALS AND METHODS: The study included 40 patients, in whom a total of 190 Southern implants were placed, 102 in maxillary sites and 88 in mandibular sites. All were loaded within 72 hours of placement. Sixteen patients were completely edentulous in the mandible and/or the maxilla. The remaining 24, who were partially edentulous, received fixed partial dentures or single-implant restorations. All of the definitive implant restorations were screw retained. The criterion for loading was clinical judgment of primary stability, verified by a «screw test.» Impressions were made after implant placement to facilitate the fabrication of a laboratory-made heat-processed provisional restoration from acrylic resin. Following a 4-month period for osseointegration and soft tissue healing, definitive fixed prostheses were fabricated. RESULTS: There were no surgical complications. After 1 to 2 years, all 190 implants had survived and were considered 100% successful, as determined by independent testing of mobility and radiographic evidence of osseointegration. In 4 patients, fracture of the provisional restoration occurred during the healing period. DISCUSSION: Clinical research has shown that immediate loading is a viable treatment modality. The favorable success rate reported in this study for rough-surfaced implants suggests that adherence to a protocol, an important parameter of which is primary stability above 32 Ncm, can lead to osseointegration. CONCLUSION: The results of this limited investigation suggest that patients who are partially or completely edentulous may be immediately restored with implants and fixed provisional restorations, provided that the dental implants are adequately stable immediately after their surgical placement. This alternative therapeutic approach did not appear to affect the up-to-2-year survival of the implants in this patient population. 6. Payne, AG, Tawse-Smith, A, Thompson, WM, Kumara, R. Early functional loading of unsplinted roughened surface implants with mandibular overdentures 2 weeks after surgery. Clin Implant Dent Relat Res. 2003; 5 (3):143-53. PMID: 14575630 BACKGROUND: Before early functional loading of unsplinted implants with mandibular overdentures can become widespread, more clinical studies are needed to investigate the success of the approach. PURPOSE: To evaluate the success rates of two types of roughened titanium surface implants with early 2-week functional loading of paired mandibular interforaminal implants with overdentures. MATERIALS AND METHODS: Random allocation divided 24 strictly selected edentulous participants into two groups, with each group to receive a different implant system (ITI Dental Implant System, Straumann AG, Walden- burg, Switzerland; or Southern Implant System, Southern Implants, Irene, South Africa). Two implants were placed in the anterior mandible of all participants using one-stage standardized surgical procedures. Previously constructed conventional mandibular dentures (opposing maxillary complete dentures) were temporarily relined and worn by the participants for the first 2 weeks; participants used a soft diet. Two weeks after implant surgery and following some mucosal healing, the mandibular dentures had the tissue conditioner removed and the appropriate matrices included for an unsplinted prosthodontic design. RESULTS: No implant from either group was lost. Resonance frequency analysis (RFA) indicated higher primary stability at surgery for the Southern group than for the ITI group, with a statistically significant difference between the groups throughout the study period. The drop in RF values between surgery and 6 weeks was significant and was greater for the Southern group. RFA also indicated stabilized osseointegration between 6 to 12 and 12 to 52 weeks, with no participant showing any decrease in those values over time. Participants with type 3 bone showed a significant improvement in RF values between 12 and 52 weeks, eventually matching those of participants with type 2 bone. There were no significant differences in marginal bone loss, periimplant parameters, or prosthodontic maintenance between the groups over the study period. CONCLUSIONS: Using only strict patient selection criteria, 1-year follow-up data indicate that early functional loading of ITI and Southern implants with mandibular two-implant overdentures is possible as early as 2 weeks after implant surgery. 7. Howes, D.G., Boyes-Varley, J.G., Lownie, J.F., The Zygomatic Implant Protocol in the treatment of the severely resorbed maxilla. SADJ 2003; 58:3; 106-114 The zygomaticus dental implant, designed by Nobel BioCare, was developed primarily for the treatment of the severely resorbed maxilla. Branemark has reported an overall success rate of 97.6% with the placement of over 200 zygomatic implants during the period 1989 to 2001. There are well-defined characteristics within the patient’s resorbed skeletal frame which guide the surgical placement of the zygomatic implant, thus determining whether the surgeon should use an implant with a 45º or 55º angulated head. This allows implant-supported restoration of the resorbed maxilla with a fixed cross arch prosthesis in the maxilla without a bone graft to the posterior maxilla. The use of a modified head angulation of 55º, with implant placement as close to the crest of the edentulous ridge as possible, allows restorative clinicians to achieve an ideal restorative position in the posterior maxilla. The use of a zygomatic implant with a 55º head reduces the buccal cantilever by 20%. 8. Watson.G.K., Payne, A.G.T., Purton, D.G., Thomson W.M. Mandibular overdentures: Comparative evaluation of prosthodontic maintenance of three different implant systems during the first year of service Int J Prosthodon 2002; 15: 259-266. PURPOSE: The purpose of this study was to evaluate the professional time required for the prosthodontic maintenance events of mandibular implant overdentures during the first year of service using three different implant systems (ITI, Steri-Oss, or Southern). MATERIALS AND METHODS: Seventy-two mandibular implant overdenture patients were allocated to three equal groups, each treated with a different implant system. Data on prosthodontic maintenance events during the first year were categorized and analyzed according to professional time allocation per procedure. RESULTS: Sixty-eight percent of the patients, regardless of implant system, required prosthodontic maintenance in the first year, most commonly for the matrices. The Southern Implants matrices required less maintenance than those of Steri-Oss or ITI (P < .05). Additional overdenture maintenance was required by 28% of patients, irrespective of implant system. When all categories of prosthodontic maintenance were combined, there were no differences between implant groups. Evaluation of overall prosthodontic success using six-field tables revealed statistically significant differences between the three implant systems, with more ITI and Steri-Oss patients than Southern Implants patients requiring overdenture retreatment (repair). CONCLUSION: During the first year of service, the matrix maintenance requirements of Southern Implants were significantly lower than those of the ITI or Steri-Oss groups; this was reflected in the number of retreatment (repair) categories recorded. Although the three systems did not differ significantly for overall prosthodontic maintenance, both the Steri-Oss and the ITI titanium matrices showed problems of clinical significance. 9. Daly P.F., Pitsillis, A., Nicolopoulos, C., Occlusal reconstruction of a collapsed bite by orthodontic treatment, pre-prosthetic surgery and implant supported prostheses: A case report. SADJ 2001; 56-6; 278-282. The loss of mandibular molars can result in a ‘collapsed bite’ owing to tilting of teeth adjacent to the gap and overeruption of maxillary molar segments. The lost interarch and interdental space must be regained before prosthetic reconstruction. This case report documents the treatment of a patient by orthodontic, surgical and prosthetic means. The teeth were orthodontically aligned to meet predetermined surgical and prosthetic requirements. The surgical phase comprised a posterior segmental maxillary osteotomy and one-stage placement of three large-diameter implants in the mandible. Finally, the occlusion was restored with mandibular implant-supported prostheses. 10. Payne, A.G., Tawse-Smith, A., Thomson, W.M., Duncan, W.D., Kumara, R. One-stage surgery and early loading of three implants for maxillary overdentures: a 1-year report. Clin Implant Dent Relat Res. 2004; 6(2):61-74. This article uses the 3.25mm diameter implant under extremely demanding conditions. BACKGROUND: Maxillary implant overdentures opposing mandibular two-implant overdentures are an underused treatment option for edentulous patients. Fewer implants, simple surgery, and short healing periods may increase patients’ acceptance of this treatment concept. PURPOSE: To determine implant success, after overdenture loading, of three narrow-diameter roughened-surface implants placed in edentulous maxillas, using a one-stage surgical procedure, a 12-week healing period, and opposing mandibular two-implant overdentures. MATERIALS AND METHODS: Forty edentulous participants with mandibular two-implant overdentures were allocated to two groups with similar implant systems. Each group had three narrow-diameter roughened-surface implants placed into their edentulous maxillas in a one-stage surgical procedure. Standardized intraoral radiography and implant stability tests were performed sequentially at surgery, at 12 weeks (prior to loading), and at 64 weeks (after 1 year of loading with maxillary overdentures). RESULTS: One hundred seventeen implants were placed in 39 participants. After 1 year of loading, 15 implants had failed in 11 patients, 4 implants have been ‘put to sleep’ in 3 patients, and 1 patient has died. Data on marginal bone loss and resonance frequency analysis showed no significant differences between the implant systems. The mean marginal bone loss was 1.30 mm (+/- 0.44 mm) from surgery to 12 weeks and 0.32 mm (+/- 0.48 mm) between 12 and 64 weeks with loading. The mean implant stability quotient and resonance frequency values showed a statistically significant improvement over time, at 56.05 (5,891 Hz), 57.54 (5,981 Hz), and 60.88 (6,167 Hz) at surgery, 12 weeks, and 64 weeks, respectively. The overall success rate for all implants combined was 81%, and the cumulative survival rate was 84.61%. CONCLUSION: In patients with mandibular two-implant overdentures, three narrow-diameter roughened-surface implants can be placed in the edentulous maxilla, using a one-stage surgical procedure, and can be loaded within 12 weeks with overdentures for 1 year. 11. Esposito M., Grusovin, M.G., Coulthard, P., Thomsen, P., Worthington, H.V. A 5-year follow-up comparative analysis of the efficacy of various osseointegrated dental implant systems: a systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants. 2005 Jul-Aug;20(4):557-68. PURPOSE: To test the null hypothesis that there is no difference in failure rates between various root-formed osseointegrated dental implant systems after 5 years of loading. MATERIALS AND METHODS: A search was conducted for all randomized controlled clinical trials (RCTs) comparing different implant systems with a follow-up of 5 years. The Cochrane Oral Health Group’s Trials Register, CENTRAL, MEDLINE, and EMBASE were searched. Several dental journals were also searched by hand. Written contacts were established with authors of the identified RCTs and with more than 55 oral implant manufacturers and personal contacts to identify unpublished RCTs. No language restriction was applied. The last electronic search was conducted on February 1, 2005. Screening of eligible studies, quality assessment, and data extraction were conducted in duplicate. Results were expressed as random effect models using weighted mean differences for continuous outcomes and relative risk for dichotomous outcomes with 95% confidence intervals. RESULTS: Ten RCTs were identified. Four of these RCTs, reporting results from a total of 204 patients, were considered suitable for inclusion. Six different implant types were compared. On a per-patient rather than a per-implant basis, there were no statistically significant differences, with the exception of more marginal bone loss around early loaded Southern implants when compared to early loaded Steri-Oss implants (mean difference -0.35 mm; 95% CI -0.70 to -0.01). However, the difference disappeared in the meta-analysis. DISCUSSION AND CONCLUSIONS: There were no clinical differences among implant systems. However, these findings are based on only 4 RCTs with few participants. More RCTs should be conducted with larger patient samples. 12. Hall J.A., Payne A.G., Purton D.G., Torr B., A randomized controlled clinical trial of conventional and immediately loaded tapered implants with screw-retained crowns. Int. Journal of Prosthodontics 2006 Jan-Feb;19(1):17-9. PURPOSE: Surgical, prosthodontic, and esthetic outcomes of conventional and immediately loaded, single, tapered, roughened-surface Southern implants in the anterior maxilla that were restored with screw-retained crowns were compared over 1 year. MATERIALS AND METHODS: Standardized surgical and prosthodontic procedures were followed and accepted criteria were used for assessment. RESULTS: There were no significant differences within or between the control and test groups for age, gender, bone quality or quantity, implant stability measurements at surgery, or implant length. CONCLUSION: After 1 year, the implants that had been immediately loaded with single provisional crowns at surgery and definitive crowns 8 weeks later were as successful as conventionally loaded 2-stage implants. 14 out of 14 implants in the delayed loaded group survived and 13 out of 14 in the immediately loaded group survived. 13. Hall J.A., Payne A.G., Purton D.G., Torr B, Duncan W.J., De Silva R.K., Immediately restored, single-tapered implants in the anterior maxilla: prosthodontic and aesthetic outcomes after 1 year. Clin Implant Dent Relat Res. 2007 Mar;9(1):34-45. BACKGROUND: Conventional implant protocols advocate a two-stage technique with a load-free, submerged healing period. Recent studies suggest that immediate restoration of single implants may be a viable treatment option. PURPOSE: The purpose of this study was to evaluate prosthodontic and aesthetic peri-implant mucosal outcomes of immediately restored, Southern single-tapered implants in the anterior maxilla after 1 year. MATERIALS AND METHODS: Participants (mean age: 43.25 years; range: 23-71 years) satisfying specified inclusion criteria were randomly allocated to conventional two-stage restoration (control group; n=14) and immediate restoration groups (test group; n =14) in a randomized controlled clinical trial. Tapered, roughened-surface Southern implants were placed using a standardized technique, and implant level bone impressions were made. Provisional screw-retained crowns, out of occlusion, were placed at second-stage surgery after 26 weeks for the conventional restoration group, and within 4 hours of implant placement for the immediate restoration group. Both groups had definitive screw-retained metal-ceramic crowns placed in occlusion 8 weeks later. Peri-implant mucosal response and papilla index were recorded 4 weeks after definitive crown placement to allow for mucosal maturation and at 1 year. Prosthodontic and aesthetic outcomes were assessed using established criteria. RESULTS: There were no significant differences within, or between, the control and test groups for age, gender, bone quality or quantity, implant stability measurements at surgery, or implant length. There were no significant differences in the implant success rate as determined by radiographic bone loss and stability tests after 1 year. There were no significant differences in prosthodontic maintenance, peri-implant mucosal response, and papilla index between the two groups over 1 year. CONCLUSIONS: Tapered, roughened-surface implants immediately restored with single provisional crowns at surgery and definitive crowns 8 weeks later were as prosthodontically and aesthetically successful as conventionally restored two-stage implants during the first year of service. Restoring single implants immediately with screw-retained crowns is an efficient procedure, but the short-term outcome is by no means superior to a conventional two-stage approach.          |